

Scoliosis: Comprehensive Guide — Types, Screening & Minimally Invasive Correction
Scoliosis: A Complete Guide from Definition to Causes
Scoliosis primarily manifests as an abnormal sideways curvature of the spine, accompanied by rotational deformity of the vertebrae themselves. Medically, the severity of the curvature is typically measured using the Cobb angle. A Cobb angle greater than 10 degrees is the diagnostic threshold for scoliosis. It is crucial to understand that scoliosis is a structural abnormality. It differs from the "hunchback" or "poor posture" that many people mistakenly associate it with. Scoliosis is not merely an aesthetic concern; it can also affect the function of internal organs.
Based on the shape of the spinal curve, common classifications include:
- C-shaped Scoliosis: A single-curve pattern.
- S-shaped Scoliosis: A double-curve pattern where the spine bends in two different directions, often seen in moderate to severe cases.
- Z-shaped Scoliosis: A multi-curve, irregular pattern, typically associated with severe spinal deformities or complex underlying conditions.

What Are the Types of Scoliosis?
Based on age and cause, scoliosis can be divided into the following main types:
-
Primary Scoliosis: Most commonly seen in adolescents, especially during growth spurts. It occurs due to unknown causes (idiopathic) or congenital skeletal abnormalities.
-
Degenerative Scoliosis: Primarily affects middle-aged and elderly individuals. It develops gradually due to the wear and tear of the spine, such as degenerating discs, osteoporosis, or spinal joint degeneration, which leads to structural imbalance.
-
Congenital Scoliosis: Caused by abnormal development of the spinal bones from birth.
| Type | Description |
|---|---|
| Primary Scoliosi |
It is most common in adolescents (80% of cases), has no known cause, and affects a higher proportion of females. |
| Congenital Scoliosis |
It is caused by abnormal development of the spinal bones at birth (e.g., hemivertebra). |
| Degenerative Scoliosi |
It occurs after age 50 due to spinal deformity caused by arthritis and osteoporosis, often accompanied by nerve compression. |
Scoliosis Severity Scale (Cobb Angle)

Self-Screening Methods for Scoliosis
Although an official diagnosis of scoliosis relies on X-ray examination, simple self-checks in daily life can help detect abnormalities early and prompt you to seek professional evaluation.
1. Adam's Forward Bend Test
-
Keep your knees straight, bend your torso forward to about 90 degrees, and let your arms hang down naturally.
-
Have someone observe your back. If one side of your spine appears raised or if there is a noticeable height difference between the two sides of your back, scoliosis may be present.

2. Posture Check in the Mirror
Stand in front of a mirror and observe whether the following body parts are symmetrical:
-
Shoulders: Are they level?
-
Waist: Are the curves on both sides even?
-
Hips: Is the pelvis tilted?
-
Shoulder Blades: Does one protrude or appear more prominent than the other?
-
Lumbar Lordosis: Is there an abnormal curve in the lower back?
-
Head Position: Is it tilted to one side?
-
If multiple abnormalities are observed, it is recommended to seek medical attention promptly for an X-ray and clinical evaluation.
Symptoms and Impacts of Scoliosis
The clinical presentation of scoliosis varies from person to person. Patients with mild curves may have no obvious symptoms, but as the condition progresses, the following may gradually appear:
-
Asymmetrical Appearance: Uneven shoulders, tilted pelvis, a raised area on the back.
-
Pain and Fatigue: Increased back or waist pain after prolonged sitting or exercise.
-
Respiratory Impact: Severe curves can compress the chest cavity, limit lung expansion, and cause shortness of breath.
-
Digestive Issues: Spinal deformation may compress abdominal organs, leading to indigestion or bloating.
-
Neurological Symptoms: Nerve compression from the vertebrae can cause numbness, tingling, or weakness in the legs.
These symptoms, if persistent, not only affect quality of life but may also cause irreversible health damage.

Consequences of Not Treating Scoliosis
Once scoliosis develops, it does not resolve on its own. Leaving it untreated carries the following risks:
-
-
For Adolescents:
-
During rapid growth spurts (puberty), the curve may worsen by 5-10 degrees per year.
-
Severe deformity affects appearance, causing psychological stress and loss of self-confidence.
-
It may lead to chest wall deformity, affecting heart and lung function.
-
-
For Adults:
-
Although progression is slower, age-related degenerative changes (arthritis, herniated discs, bone spurs) can worsen symptoms.
-
Chronic back pain and nerve compression can lead to leg numbness and weakness.
-
In severe cases, walking may become difficult, potentially requiring assistive devices.
Therefore, Dr. Chien-Chun Chang and his team recommend that early monitoring and proactive treatment are key to preventing the condition from worsening.
-
-
Treatment Options for Scoliosis
The treatment approach is determined based on the patient's age, Cobb angle, severity of symptoms, and skeletal maturity.
Non-Surgical Treatment
Exercise Therapy: Specific spinal stabilization exercises (e.g., the Schroth Method) can help improve posture and muscle balance.
Bracing: Suitable for adolescents with curves between 25-40 degrees, aiming to slow progression.
Pain Management: Includes physiotherapy, heat therapy, medication, etc.
Surgical Treatment
Surgery is generally recommended when the Cobb angle exceeds 45-50 degrees, or if there is nerve compression or impaired organ function.

Minimally Invasive Navigated Scoliosis Correction Surgery
Traditional scoliosis surgery requires a large incision in the back, causing significant damage to muscles and tissues and resulting in a slow recovery. In contrast, modern medical technology has developed 3D computer-navigated minimally invasive surgery, which allows for precise correction through much smaller incisions.
Surgical Features
-
Precise Navigation, Reduced Risk: Real-time 3D imaging assists in screw placement, helping to avoid damage to nerves and major blood vessels.
-
Suitable for Curves Under 80 Degrees: This technique is applicable for moderate scoliosis.
-
Eliminates Need for Long-Term Rehabilitation: Patients can typically get out of bed within 1-3 days after surgery and be discharged from the hospital in 5-10 days, with intraoperative real-time 3D computer navigation imaging guidance.
-
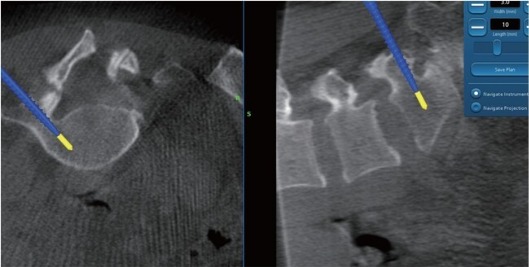
Intraoperative real-time 3D computer navigation imaging guidance
-

O-arm navigation system
OLIF: A New Minimally Invasive Surgical Option
OLIF (Oblique Lateral Interbody Fusion) is a minimally invasive spinal fusion procedure performed through the front/side of the abdomen:
-
Incision only 4 cm, avoiding the back muscles to reduce postoperative pain.
-
Shorter surgery time, less blood loss, faster recovery.
-
When combined with a navigation system, it further enhances surgical precision and safety.
International Demonstration and Training Center


Scoliosis FAQ
Q: What is scoliosis?
Scoliosis is an abnormal sideways curvature of the spine accompanied by rotation of the vertebrae. It is diagnosed when the Cobb angle exceeds 10 degrees. It is not merely poor posture but a structural abnormality that can affect appearance, nerve function, and cardiopulmonary health.
Q: Can I self-check for scoliosis?
Yes. Common self-screening methods include the Adam's Forward Bend Test and checking your posture in a mirror to observe symmetry in the shoulders, waist, pelvis, and shoulder blades. If you notice significant asymmetry, it is recommended to seek a medical evaluation promptly.
Q: What happens if scoliosis is left untreated?
Scoliosis does not resolve on its own. Without treatment, it can progress rapidly in adolescents, affecting appearance and cardiopulmonary function. In adults, degenerative changes can lead to chronic pain, nerve compression, and potentially even difficulty walking.
Q: When is surgery recommended for scoliosis?
Surgery is typically recommended when the Cobb angle exceeds 45–50 degrees, when there are symptoms of nerve compression, or when the curvature impairs cardiopulmonary function. Surgical options include traditional open surgery or 3D computer-navigated minimally invasive surgery.
Q: What are the advantages of OLIF minimally invasive surgery?
The OLIF procedure is performed through the front/side of the abdomen, avoiding the back muscles. It offers a small incision, minimal blood loss, less pain, and a faster recovery. When combined with computer navigation, it further enhances surgical precision and safety.
Q: Is rehabilitation needed after scoliosis surgery?
Most patients undergoing minimally invasive scoliosis correction can get out of bed within 1–3 days and be discharged in 5–10 days. Long-term rehabilitation is usually not required, but patients must follow their doctor's guidance on posture and activity adjustments
.
A Reminder from Dr. Chien-Chun Chang's Team
Scoliosis is a common condition, but early detection, correct assessment, and appropriate treatment can help most patients maintain a good quality of life. The combination of modern minimally invasive surgery and computer navigation technology has made treatment safer, more precise, and allows for quicker recovery. If you or a family member has concerns about scoliosis, seek advice from a spine specialist as soon as possible to determine the optimal timing for correction.